

The arrival of GLP-1 receptor agonists has undeniably reshaped obesity and diabetes management. Few therapies in recent decades have generated such rapid clinical adoption, patient demand, and media enthusiasm.
Yet amid this acceleration, an uncomfortable but necessary question is emerging:
👉 Are we solving obesity — or pharmacologically managing appetite while neglecting long-term metabolic resilience?
📉 The Sustainability Challenge
Clinical trials and post-treatment follow-ups are now painting a consistent picture:
• Significant weight loss occurs during treatment
• Discontinuation commonly results in weight regain
• Cardiometabolic improvements frequently reverse
This is not a drug failure — it reflects biology.
When pharmacological appetite suppression is removed without metabolic rehabilitation, compensatory mechanisms re-emerge.
For clinicians, this reframes GLP-1 therapy from:
“Treatment course” → “Potentially indefinite management.”
🧠 Appetite Suppression ≠ Metabolic Restoration
GLP-1 therapies effectively reduce energy intake.
However, they do not inherently correct:
• Insulin resistance drivers
• Poor dietary composition
• Protein inadequacy
• Lean muscle preservation
• Nutrient density deficits
• Behavioural eating patterns
Without structured intervention, many patients experience:
⚠️ Reduced food intake
⚠️ Reduced protein intake
⚠️ Progressive lean mass loss
⚠️ Fatigue and reduced vitality
Weight loss alone is not synonymous with improved metabolic health.
🧬 The Lean Mass Concern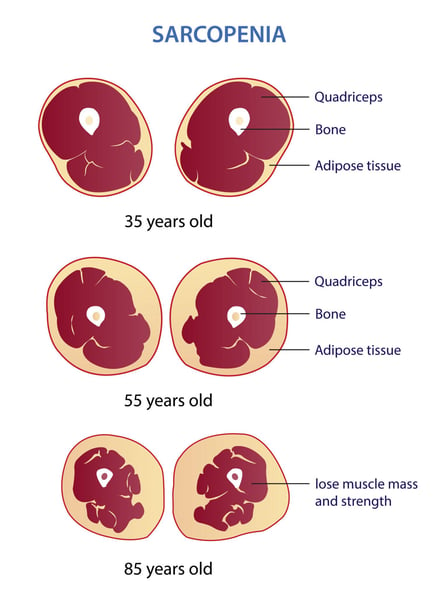
Emerging analyses suggest a proportion of GLP-1-induced weight loss may include lean muscle tissue, not purely adipose reduction.
This raises important implications:
• Basal metabolic rate decline
• Functional strength reduction
• Increased frailty risk (particularly older adults)
• Greater difficulty maintaining weight loss post-therapy
Muscle is not cosmetic tissue — it is a metabolic organ.
Loss of lean mass undermines long-term weight stability.
⚠️ Nutritional Risk: The Silent Variable
Reduced appetite frequently leads to reduced nutritional adequacy, particularly when:
• No dietary education is provided
• Patients default to convenience foods
• Meal skipping becomes routine
• Protein intake falls
Documented concerns include:
• Micronutrient insufficiencies
• Protein deficits
• Sarcopenic progression
• Poor recovery post-cessation
Pharmacotherapy without nutritional strategy introduces preventable risk.
💸 Economic & Ethical Considerations
With many patients now advised that therapy may need to be long-term or lifelong, additional questions arise:
👉 Cost sustainability
👉 Access equity
👉 Psychological dependency
👉 Exit strategy planning
If cessation predictably results in regain, clinicians must ask:
“What is the patient’s pathway beyond the prescription?”
🧩 The Clinical Gap: Where Lifestyle Must Re-Enter
GLP-1 therapies may be powerful tools.
But tools require frameworks.
Evidence increasingly supports combining therapy with:
✔️ Structured nutritional protocols
✔️ Protein optimisation
✔️ Muscle preservation strategies
✔️ Behavioural coaching
✔️ Metabolic education
✔️ Long-term weight maintenance planning
Without this integration, patients risk cycling through:
Drug → Loss → Stop → Regain → Restart
Meet Malcolm Today!
.jpg?width=329&height=439&name=Malcolm%20New%20Headshot_%20(1).jpg)
Founder and General Manager of UltraLite Progam
Join UltraLite Today!
For 26 years, UltraLite’s healthy ketogenic program has changed lives. Join the success stories—or step up and help others succeed as an UltraLite practitioner.
.jpg?width=424&height=282&name=Untitled%20design%20(1).jpg)



